Pediatric Cavernous Sinus Syndrome as the Initial Presentation of Intracranial Germinoma: A Case Report-Juniper Publishers
Abstract
8-year girl complained of diplopia and her right eye presented ptosis, supraduction, abduction deficit, slight esotropia, and corneal hypoesthesia. Visual acuity was 20/20 in both eyes. Pupillary light reflex showed full, fast constriction and afferent pupillary defect was negative. No optic disc abnormalities were observed and indicated cavernous sinus syndrome. A brain magnetic resonance imaging indicated a tumor lesion from the sellaturcica to the suprasellar region and advancing into the right cavernous sinus, compressing the optic chiasm. Tumor biopsy was performed. Histo pathological examination led to a diagnosis of intracranial germinoma. Intracranial germinoma manifest hypopituitarism and bitemporal hemianopsia but in this case, intracranial germinoma manifesting as cavernous sinus syndrome initially. Cavernous sinus syndrome represents highly in adults and pediatric cases are rare. Malignant lymphoma and Trosa-Hunt syndrome were occasionally reported as diseases causing cavernous sinus syndrome in children. But, to our knowledge, there were a few reports of intracranial germinoma. Although it is very rare, germinoma should be kept in mind as a disease which causes cavernous sinus syndrome in children.
Introduction
8-year-old girl complained of diplopia from April
2006, and started tilting her head to see things. Intermittent ptosis of
the right eye appeared in May. Because right eye movement disorder was
noted, she initially visited our department on October. The visual
acuity was 20/20 in both eyes, the light reaction was complete and
rapid, and relative afferent pupillary defect (RAPD) was negative.
Ptosis of the right eye was noted. The pupil diameters were 4.6 and
3.7mm on the right and left sides in a bright room, respectively, and
4.6 and 5.7mm in a dark room, respectively, showing laterality. The
pupil diameter after a cocaine eye drop test were 4.5 and 5.7mm in a
bright room, respectively, being judged as positive for the test.
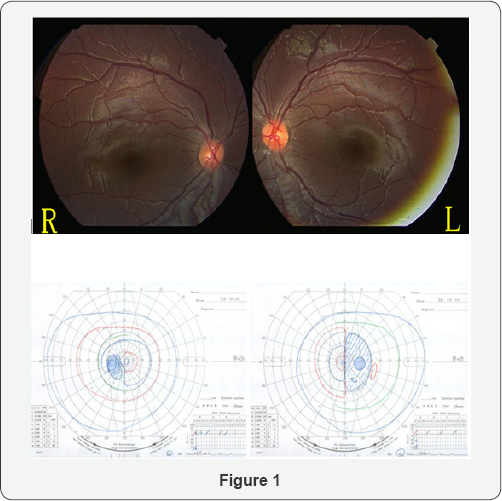
Regarding eye movement, impairment of abduction and supraduction, mild
impairment of adduction, and infraduction disorder of the right eye were
observed, and corneal sensory reflex of the right eye was reduced. No
abnormality was noted in the anterior segment of the eye, optic media,
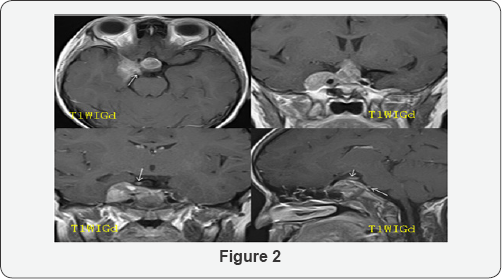
or fundus.Bitempolal hemianopia in visual field was observed (Figure 1). On brain magnetic resonance imaging (MRI) performed (Figure 2),
a mass lesion advancing from inside the sellaturcica to the supra
sellar region and right cavernous sinus was observed. Contrast
enhancement of the tumor continuous from the right cavernous sinus was
observed, and it advanced along the oculomotor and abducens nerves, the
serum human chorionic gonad otropin-β (hCG-β) level was high suggesting
germ cell tumor. Regarding the systemic condition, panhypopituitarism
was present, and hormone replacement therapy was initiated. Tumor biopsy
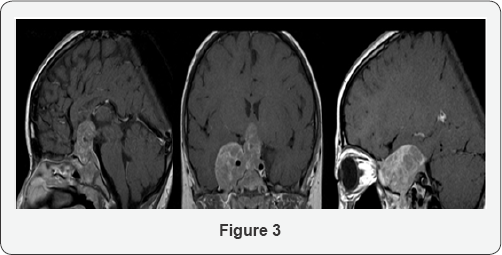
was scheduled but it was postponed by her family. The visual acuity of
the left eye decreased to 20/50 in February 2007, and impairment of
supraduction of the right eye aggravated. On MRI performed in the same
period (Figure 3),
compression of the chiasma became stronger in the suprasellar region.
On the right side, the tumor advanced along the orbital apex and
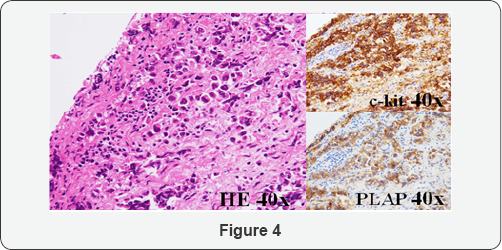
trigeminal nerve. Tumor biopsy by craniotomy was performed on March 6,
2007. Solitary appearance of large cells containing bright and wide
cytoplasm was observed on histopathological examination (Figure 4),
and cells were positive for placental alkaline phosphatase (PLAP) and
c-kit on immunostaining. Based on these findings, the tumor was
diagnosed as intracranial germinoma. Radiotherapy and chemotherapy were
immediately performed, and the tumor shrank. On follow-up in July, the
visual acuity became 20/20 in both eyes, and the tumor has not recurred
for 8 years.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
In the present patient, diplopia and ptosis were the initial symptoms and the features of cavernous sinus syndrome complicated by Horner's syndrome were observed. These clinical findings were consistent with the mass lesion advancing from inside the sellaturcica to the suprasellar region and right cavernous sinus observed on MRI. To our knowledge, only 3 cases [1-3], of intracranial germinoma causing cavernous sinus syndrome as the initial symptoms. In these 3 cases, the tumor was heterogeneously enhanced with gadolinium on MRI and Serum or cerebrospinal fluid hCG-β was positive.One case is children [1]. 11-year-old girl presented of left 6th cranial nerve Palsty without visual field defect. Her head MRI showed a mass mainly located in the left cavernous sinus. First biopsy want clearly histlogycal evidence of tumor cells. Intracranial germinoma was diagnosed by second biopsy five month later. Retrospective analysis of the first specimen revealed a few cells positive for c-kit immune histo chemical stain. Thus c-kit is useful for the differential diagnosis and might have resulted in early diagnosis at the first exploration. Present case test of c-kit, hCG-β and PLAP were positive in serum or cerebro spinal fluid, so we could suspect for intracranial germinoma.
Intracranial germinoma accounts for 15% of pediatric
tumor cases and it is higher in Japan than in the other western
countries (3-4%) [4].
It arises in the pineal body and suprasellar regions and induces
various symptoms. Clinical manifectation are hypopituitarism and
bitemporal hemianopsia. In this case, intracranial germinomam anifesting
as cavernous sinus syndrome initially. Most cases occuring cavernous
sinus syndrome develop in adults and pediatric cases are rare. Malignant
lymphoma [5,6] and Trosa-Hunt syndrome [7-9]
were occasionally reported as diseases causing cavernous sinus syndrome
in children. Although it is very rare, intracranial germinoma should be
kept in mind as a disease which causes cavernous sinus syndrome in
children.
For more Open Access
Journals in Juniper Publishers please
click on: https://juniperpublishers.com
For more articles in JOJ Ophthalmology (JOJO) please click on: https://juniperpublishers.com/jojo/index.php
For more about juniper publishers please click on:
https://www.juniperpublishersgroup.com/