Nasolacrimal Duct Obstruction Review-JOJ Ophthalmology
Introduction
The lacrimal system comprises two components the main and accessory lacrimal glands and their secretions and the lacrimal excretory system [1]. The lacrimal excretory system is divided into the proximal and distal sections. The proximal section includes the punctum, canaliculus, and the common canaliculus [2,3]. The distal lacrimal drainage system consists of the lacrimal sac and the nasolacrimal duct that finally ends under the inferior turbinate and empties into the inferior meatus [2].
The precorneal tear film is composed of aqueous, mucinous and oily components and is necessary for the maintenance of the cornea as well as the maintenance of the ocular surface epithelium. More than 90% of the lacrimal fluid is removed by the excretory system, whereas less than 10% evaporates between blinks. Outflow is mainly regulated by the pumping effect of the orbicularis oculi muscle (Horner muscle) [3,4]. Tears are thus drawn into the lacrimal excretory system after each blink. The passage of tears down the nasolacrimal duct is influenced by gravity, evaporation in the nose, and inspiration and expiration.
Diagnosis
A detailed history of any systemic or topical medication, surgery, trauma or scarring, and infection must be obtained. It is valuable to grade the severity of epiphora using a uniform grading system such as the Munk scale [5]. Slit lamp examination starts with recognizing the papilla, presence of a membrane or fibrosis over the punctum, punctum size, tear meniscus height, eyelid margin, conjunctiva around the punctum, eyelid malposition, position of the punctum in the tear lake, and any sign of previous surgery. The Schirmer test [6], tear break up time [7], ocular surface staining, and tear meniscus height will rule out any associated ocular surface abnormalities. Abnormal dye disappearance test is a very maneuver to assess abnormal tear drainage system and is especially helpful in pediatric patients [7].
Congenital Nasolacrimal Duct Obstruction
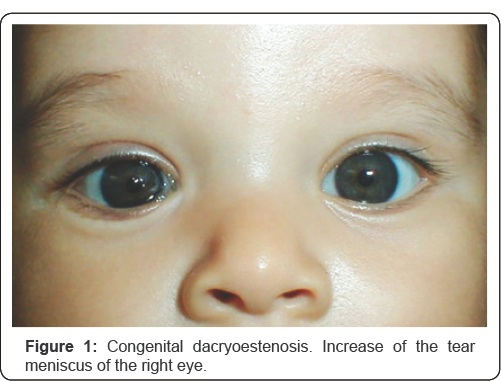
Congenital nasolacrimal duct obstruction is the first cause of pediatric epiphora. Other causes include congenital punctum and canaliculus stenosis and/or atresia, nasal malformations and craneofacial abnormalities. It is frequently seen at birth due to lack of perforation of the valve of Hasner or an inferior and distal nasolacrimal duct opening failure. At birth, half of the nasolacrimal new born pathways are not permeable. A spontaneous apoptosis mechanism takes place between 3rd- 4th weeks after birth. Nevertheless, the obstruction persists in approximately 20% of the patients. Symptoms of congenital nasolacrimal duct obstruction consist of epiphora and dacryocystitis. The diagnosis is easily made in the office by observing epiphora and mattering of the eyelashes (Figure 1). It can be confirmed by compression over the nasolacrimal sac, which results in regurgitation of mucopurulent material in those patients who have developed chronic dacryocystitis. Instillation of 2% fluorescein dye and observation of abnormally delayed passage from de cul-de-sac is helpful in confirming the diagnosis.
{kind=link}
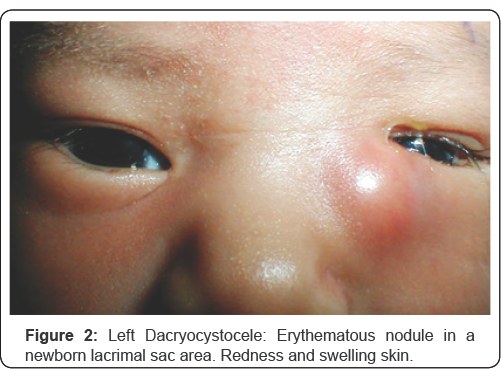
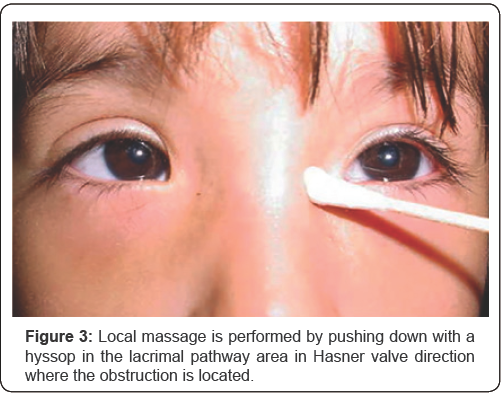
This is a rare entity presented at birth or within the fourth week after birth. The blockage Rosenmüller valve. An edematous, tender and red mass below the medial canthal tendon will be clinically found (Figure 2). Conservative management (medical treatment). If dacryocele is initially sterile, all patients must be treated with warm compresses, local massage and topical antibiotics [8]. Those infected will be treated with broad spectrum intravenous antibiotic therapy [9]. Local massage by pushing down the lacrimal sac is useful and accelerates the lumen duct perforation process (Figure 3). Controversy exists whether conservative management or early probing for decompression are preferable.
{kind=link}
{kind=link}
Surgical Management of Congenital Nasolacrimal Obstruction
Probing consist by introducing a thin metal probe into the lacrimal punctum trough the nasolacrimal pathway, producing a mechanical opening in the obstruction site. It is an operating room procedure under general anesthesia. The ideal time is controversial, most of the time the procedure is performed around the first year of life for those patients that did not show spontaneous improvement or despite conservative treatment [10].
Close dacryointubation is performed by placement of silicone stents through the superior and inferior canaliculus and down to the nasolacrimal duct. This dilates the inferior meatus. The duration of the stent employment ranges from 6 weeks to 6 months [10]. Dacryocystorhinostomy surgical procedure involves the removal of bone adjacent to the lacrimal sac draining directly into the nasal cavity and it is performed when siliconte intubation have failed.
Differential Diagnosis
Dermoid cyst, dongenital glaucoma, acute conjunctivitis, corneal abrasion, trichiasis, ocular foreign body sensation and meningoencephalocele must be discarded.
Acquired Nasolacrimal Duct Obstruction
The primary acquired nasolacrimal duct obstruction is caused by inflammation or fibrosis without any precipitating cause. Appears in middle age and elderly females in 3:1 ratio. The obstruction site is located in the lower nasolacrimal fossa and middle nasolacrimal duct. The secondary acquired obstruction is caused by inflammation or fibrosis with precipitating causes as infectious, inflammatory, neoplastic, traumatic or mechanical factors [11,12].
Clinical presentation Patients with primary acquired nasolacrimal duct obstruction most commonly present with a history of epiphora. A chronic dacryocystitis owing to tear stasis can show a mucopurulent discharge at the punctum, or pus can be expressed from the punctum by massage of the lacrimal sac. Two stages can be distinguished [13].
Acute Dacryocystitis
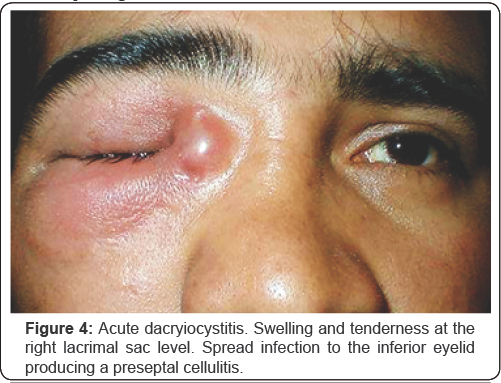
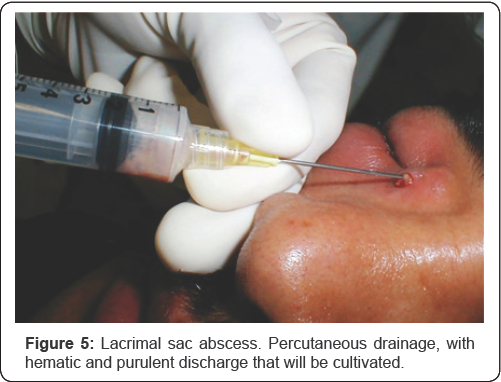
Is an acute inflammation of the lacrimal sac due mostly to the obstruction of nasolacrimal duct. In most cases is a clinical diagnosis. Lacrimal sac bacterial overgrowth and inflammation? occludes the superior and the natural drainage creating a true abscess. Symptoms and signs include a no compressible painful and erythematous mass below the medial canthal tendon. Medical treatment must be initiated because of the risk of extension to the periocular tissues and the orbit (Figure 4 ) including topical and systemic antibiotics, analgesics and antiinflammatory measures. Local heat and massages helps drainage and the opening of the obstruction siteLacrimal sac abscess requires sometimes manual percutaneous drainage, material can be collected and cultivated (Figure 5). Avoid irrigation during the acute phase because the risk of dissemination of the infectious process. Definitive treatment is a dacryocystorhinostomy procedure which can be performed as an external or internal endoscopic. It is preferable to postpone two or three weeks after the acute phase resolution.
{kind=link}
{kind=link}
Chronic Dacryocystitis
Symptoms and signs include recurrent epiphora, swelling and redness at medial canthus and a painless and compressible mass below the medial canthal tendon. The patient usually refers history of previous acute dacryocistitis or chronic unilateral conjunctivitis.
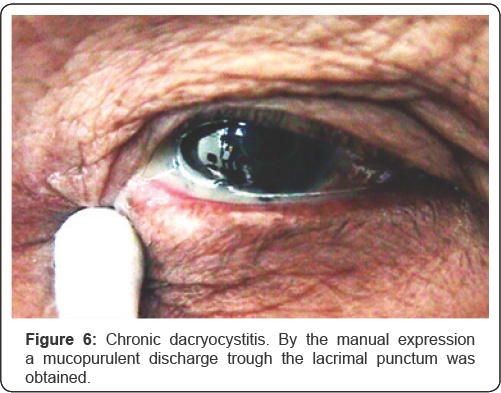
The lacrimal sac is filled with mucoid or purulent discharge that can be expressed frequently with local massage (Figure 6). Medical treatment includes topic and systemic antibiotics and a dacryocystorhinostomy as the surgical first choice. Differential Diagnosis: Preseptal cellulitis, sinusitis, canaliculitis, sebaceous cyst and neoplastic tumours.
{kind=link}
Conclusion
For most tearing patients a diagnosis can be arrived at after a thorough history and a few relatively simple office procedures. A small number of cases will require more sophisticated studies to confirm the site of anatomic block. With the various test available, appropriate medical or surgical management can be determined in the vast majority of patient with tear production and drainage imbalance. Nasolacrimal duct obstruction is a common finding and the ophthalmologist must be prepared to recognize signs and symptoms to perform an accurate diagnosis and offer a correct management.
For more Open Access
Journals in Juniper Publishers please
click on: https://juniperpublishers.com
For more articles in Journal
of Physical Fitness, Medicine & Treatment in Sports
please click on: https://juniperpublishers.com/jpfmts/index.php
For more about juniper publishers please click on: https://www.juniperpublishersgroup.com/
I have been absent for some time, but now I remember why I used to love this web site. Thanks , I’ll try and check back more often. How frequently you update your site?astigmatism circle lenses
ReplyDelete