Keratoconus Progression Diagnosis Evidenced by Corneal Epithelium Mapping-Juniper Publishers
Case Report
Background
We are reporting a case of a 16y.o. (y.o.b. 1996) young gentleman that we have followed for keratoconus in our center about a year ago. His first visit occurred on February, 2011. At this time he was informed about the different options such as collagen cross-linking, INTACS, the Athens Protocol (the combination of topography-guided partial ablation PRK with CXL), and lamellar keratoplasty. Following a complete clinical investigation, recommendation was given that the 0S be treated with cross-linking with simultaneous partial topography-guided excimer surface ablation (Athens Protocol) [1], which was performed in May, 2011.
The 0D had reasonable good correction (BCVA 20/20) and therefore, due to his age and good corneal thickness (CCT in the vicinity of 500μim), we recommended for him to follow eight months to a year's time in order to evaluate a possible progression and the possibility of intervention. This paper is about our investigation of the 0D keratoconus progression not only by optical anterior segment imaging technologies, but also by the epithelium mapping, which supported our findings relating to correlation of keratectasia and elevated corneal overall epithelium.
Methods and technologies
Anterior-segment imaging of keratometric, topometric and topographic parameters can be an important tool in the decisionmaking process and prompt action. The optical instruments involved in this report were Biometry by I0L Master (Carl Zeiss Meditec Inc., USA), Anterior-Segment 0ptical Coherence Tomography (AS OCT) by Optovue RTVue (Optovue Inc. Fremont, CA), Placido topography and Scheimpflug topography by Wave light (Erlagen, Germany), specifically the Topolyzerand the Pentacam High Resolution (Oculus Optikgerate GmbH), a.k.a. Oculyzer II, which is a Pentacam HR that has been specially configured to export topometric data to Alcon's refractive suite [2]. The ultrasound bio microscopy (UBM) instrument was the Artemis II + superior (Artemis Medical Technologies Inc. Vancouver, British Columbia, Canada) [3]. To our knowledge this is the first such documented case combining these optical modalities with epithelium mapping by HF ultrasound for keratoconus screening in the peer-reviewed literature.
Patient follow-up
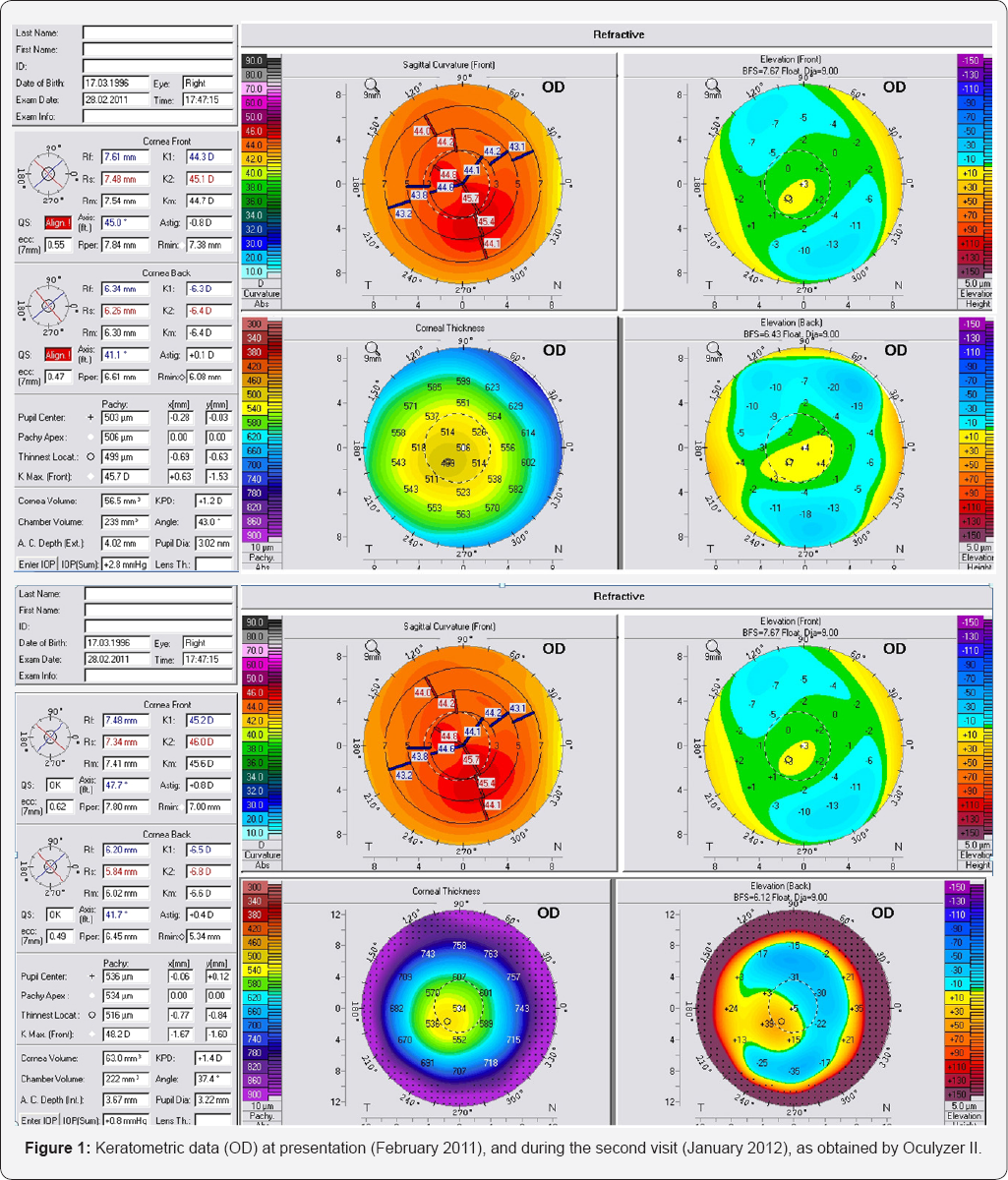
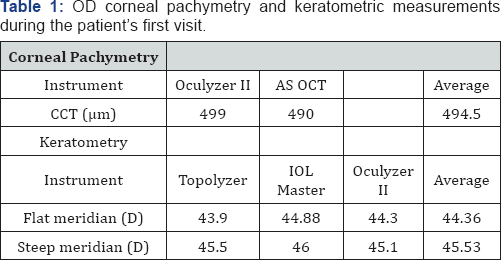
The initial anterior segment parameters recorded during the first visit (late February, 2011) are summarized in (Figure 1 &Table 1). Based on these findings, astigmatism was determined -1.25 D, with the flat axis was determined at 21°. We saw the patient several months later (late January, 2012). The data (Figure 2 & Table 2), indicated keratoconic progression, despite that overall corneal thickness was found increased by an average of 13μim. For example, the difference with the Pentacam (Oculyzer II) preimposed on the old and newer topometric measurement showed a change in the central steepening. For example, sagittal curvature increased, K1 (flat axis) by +0.2 D and K2 (steep axis) by +0.8 D. Likewise, anterior surface elevation was found increased by approximately + 13μim, also there was change between lowest elevation to pupil center (20711, -13 -> +3μiM, 2012 -18 -> +8μim). Based on these findings, astigmatism was determined at 40°
{kind=link}
{kind=link}
{kind=link}
{kind=link}
We decided to further evaluate this finding because on topometric terms this finding suggested progression of the keratoconus. We obtained Artemis II+ HF UBM corneal epithelium mapping. Careful evaluation of the UBM findings revealed that the epithelium (Figure 3) was overall thicker compared to a population of 33 patients (50 eyes) [4]. The patient’s epithelium featured mean thickness 56μm (normal population 50.8μim), central thickness 60μm (normal population 52.1μm), and average peripheral thickness 50μm (normal population 49.54μm), while over the cone (located superiorly - temporal) the epithelium was thicker, at 53μm.
{kind=link}
Discussion
We feel that this is a good example where the -at first sight- progression of keratoconus is accompanied by epithelium whose thickness is overall thicker than the control population, particularly at the pupil center by a significant amount (+8μm). This would be impossible to establish with Scheimpflug imaging maps alone. It appears the HF Ultrasound is able, by giving the specific epithelium maps to point to that direction. Obviously, for the definite diagnosis of this theory would be re-evaluation of the cornea with Oculyzer and UBM. In case where the epithelium returned to a thinner thickness we would expect that the Pentacam maps would flatten and that would establish that there is no actual progression of the keratoconus. It is interesting to compare the posterior curvature maps of past and current and see in these maps that there is a change in posterior curvature. One has to take into account that the increase of irregularity by the epithelium thickening may be the factor that creates this bias.
Acknowledgement
Dr. Kanellopoulos is a Consultant to Alcon Wave light.
For more Open Access Journals in Juniper Publishers please click on: https://juniperpublishers.com
For more articles
in JOJ
Ophthalmology (JOJO) please click on: https://juniperpublishers.com/jojo/index.php
For more about juniper publishers please click on: https://www.juniperpublishersgroup.com/
No comments:
Post a Comment