JUNIPER
PUBLISHERS- JOJ Ophthalmology
Abstract
A 77 year old man presented with worsening vision and
a history of diabetic retinopathy with previous intravitreal
injections. Fundus examination showed diabetic macular edema in the
right eye and bilateral moderate non proliferative diabetic retinopathy.
It was decided to start treatment with the anti-Vascular Endothelial
Growth Factor Bevacizumab (Avastin®). After multiple Avastin injections
in OD, fundus examination revealed previously unobserved silicone oil
bubbles in the eye. Patient denied noticing any visual interference from
the silicone bubbles, and continued receiving his scheduled Avastin
injections with close monitoring. Silicone oil accumulation in this
patient may be the result of the lubricant used in the syringes during
his intravitreal injections. These silicone oil droplets have persisted
in the patient’s vitreous chamber, though their long term effects are
unknown. Further studies are needed to assess the long term safety of
silicone oil accumulation secondary to intravitreal injections.
Keywords: Silicone oil; Avastin; Bevacizumab; Lucentis; Eylea; Droplet; Injection; Intraocular; Intravitreal; Bubbles; SyringeIntroduction
Intravitreal injection use has increased markedly
with the discovery of agents that can hinder the progression of many
vascular endothelial growth factor (anti-VEGF)-mediated diseases,
including choroidal neovascularization, diabetic macular edema (DME),
diabetic retinopathy and retinal venous occlusive disease. There are
many procedure-related complications of intravitreal injections,
including damage to the lens, sterile and infectious endophthalmitis,
retinal tears, retinal detachment, intraocular inflammation and vitreous
hemorrhage. We report a case of intravitreal silicone oil bubbles found
in the eye of a patient after receiving multiple Avastin injections.
Case Report
A 77 year old man with a history of hypertension,
type 2 diabetes mellitus, deep vein thrombosis and pulmonary embolism on
anticoagulation medication presented with gradually progressing loss of
vision in his right eye. His ophthalmologic history is significant for
right sided cataract removal, bilateral primary open angle glaucoma
treated with Dorzolamide-Timolol and Bimatoprost, moderate non-
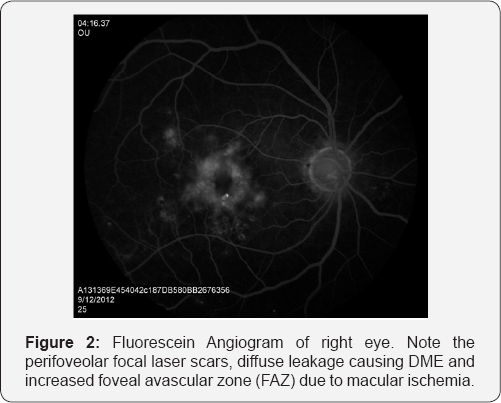
proliferative diabetic retinopathy (Figure 1 & 2) and diabetic macular edema requiring multiple Avastin injections.
{kind=link}

Evaluation revealed visual acuity of 20/400OD and
20/20OS, and intraocular pressure was 11mmHg OD and 13mmHg OS. Dilated
fundus examination revealed right sided macular ischemia and diabetic
macular edema, along with bilateral, moderate nonproliferative diabetic
retinopathy. During the retina exam, silicone oil bubbles in the
vitreous cavity were noticed as seen in Figure 3.
The patient’s right diabetic macular edema was treated with an Avastin
1.25mg/0.5ml injection. Upon follow-up 4 weeks later, the patient
reported vision improvement in his right eye to 20/200 so it was decided
to continue with Avastin injections to attain the resolution of his
diabetic macular edema. Patient denied awareness of silicone bubbles on
his vision test. Given that no visual deficits or pathology were
identified, no further interventions were warranted, and patient
continued with his previous schedule of care.

Discussion
Macular edema secondary to microaneurysms is the primary mechanism by which vision loss occurs in diabetic retinopathy [1].
Current treatment options include intravitreal injections of anti-VEGF
agents, steroids, and laser management. Steroids induced glaucoma, and
the limitations of using laser treatment in parafoveal microaneurysms
favor the use of anti-VEGF agents such as Bevacizumab (Avastin),
Ranibizumab (Lucentis) and Aflibercept (Eylea) [2].
Avastin injection formulations do not contain
silicone oil. Rather, silicone oil is a syringe lubricant, which may
eventually build up in the eyes of patients undergoing numerous
injections. Certain staked-on syringe designs may increase the risk of
silicone oil accumulation, while other luer syringes may lessen this
risk. In a study by Scott et al. [3]
staked-on syringe and luer designs were compared for silicone oil
residues in the eye after Triamcinolone Acetonide injections. In
patients receiving only luer cone syringe injections, no silicone oil
droplets were found, while the patients receiving injections only with
staked-on syringes were found to have silicone oil droplets in 44% of
the cases examined. These results were attributed to a 50μL residual
space in the needle hub which “squeegeed” silicone oil from the needle
as the plunger was pushed down. Others have estimated oil expulsion on
the plunger tips of disposable staked-on syringes at around 24% of the
silicone lubricant [4] with between 0.15mg and 0.25mg of silicone oil ejected after three plunger pushes to expel air droplets [5].
Handling of syringes may also be a factor, especially
the repackaging, shipping, and handling of injectables. A study by Liu
et al. [6]
found that freeze-thawed samples of injectable Bevacizumab, along with
samples that were mechanically disturbed (via dropping of package), led
to large increases in intravitreal silicone oil findings. The authors
posited that the plastic syringes into which Bevacizumab is often
repackaged were not designed to deliver intra-ocular injections, with
looser parameters for the silicone oil lubricant.
Although intraocular silicone oil has been associated
with a number of ocular diseases in larger volumes, the effects of
smaller volumes has not yet been sufficiently studied. Relatively small
injections may induce keratopathy, movement of silicone oil into the
anterior chamber, and emulsification [7].
However, larger amounts may lead to elevated post-surgical intraocular
pressure, pupillary block, angle closure with pupillary block, and
idiopathic closed-angle glaucoma. Long-term intraocular silicone oil
exposure may be associated with optic nerve damage, including
demyelination and vacuoles, along with retinal damage [8].
These changes are associated with the larger volumes of oil used in
retinal surgeries, but have yet to be found in the smaller volumes used
in intra-ocular injections.
Silicone oil may also have pharmacokinetic effects, slowing down bevacizumab distribution to ocular tissues in rabbit eyes [9].
Indeed, the efficacy of a number of drugs (e.g. insulin) may be
compromised by silicone oil. Although it is unlikely that the relatively
small volumes of silicone oil in intra-ocular injections would produce
detectable effects, care should be taken when monitoring patient
progress.
Conclusion
This case illustrates the rare yet predictable
potential for intraocular silicone oil buildup following multiple
Avastin injections. Recognition of the risk factors for intravitreal
silicone oil accumulation and close monitoring following injections may
foreclose the risk of potential negative side effects.
For more articles in JOJ Ophthalmology (JOJO) please click on: https://juniperpublishers.com/jojo/index.php
No comments:
Post a Comment